Skip to content
About
Our Doctors
Our Advanced Practice Providers
News
Careers
Clinical Trials
Sponsors
Currently Enrolling Trials
Clinical Trials FAQs
Services
Diabetes
Thyroid Disorders
Osteoporosis & Fracture
Heart Disease Prevention
Liver Health Testing
Pituitary & Adrenal Disorders
Medical Weight Loss
PCOS
Testosterone Replacement Therapy
Gender-Affirming Hormone Therapy
Patients
Patient Center
Make an Appointment
Pay my Bill
Patient FAQs
Contact
Portal
About
Our Doctors
Our Advanced Practice Providers
News
Careers
Clinical Trials
Sponsors
Currently Enrolling Trials
Clinical Trials FAQs
Services
Diabetes
Thyroid Disorders
Osteoporosis & Fracture
Heart Disease Prevention
Liver Health Testing
Pituitary & Adrenal Disorders
Medical Weight Loss
PCOS
Testosterone Replacement Therapy
Gender-Affirming Hormone Therapy
Patients
Patient Center
Make an Appointment
Pay my Bill
Patient FAQs
Contact
Portal
Request Appointment
Category: Osteoporosis
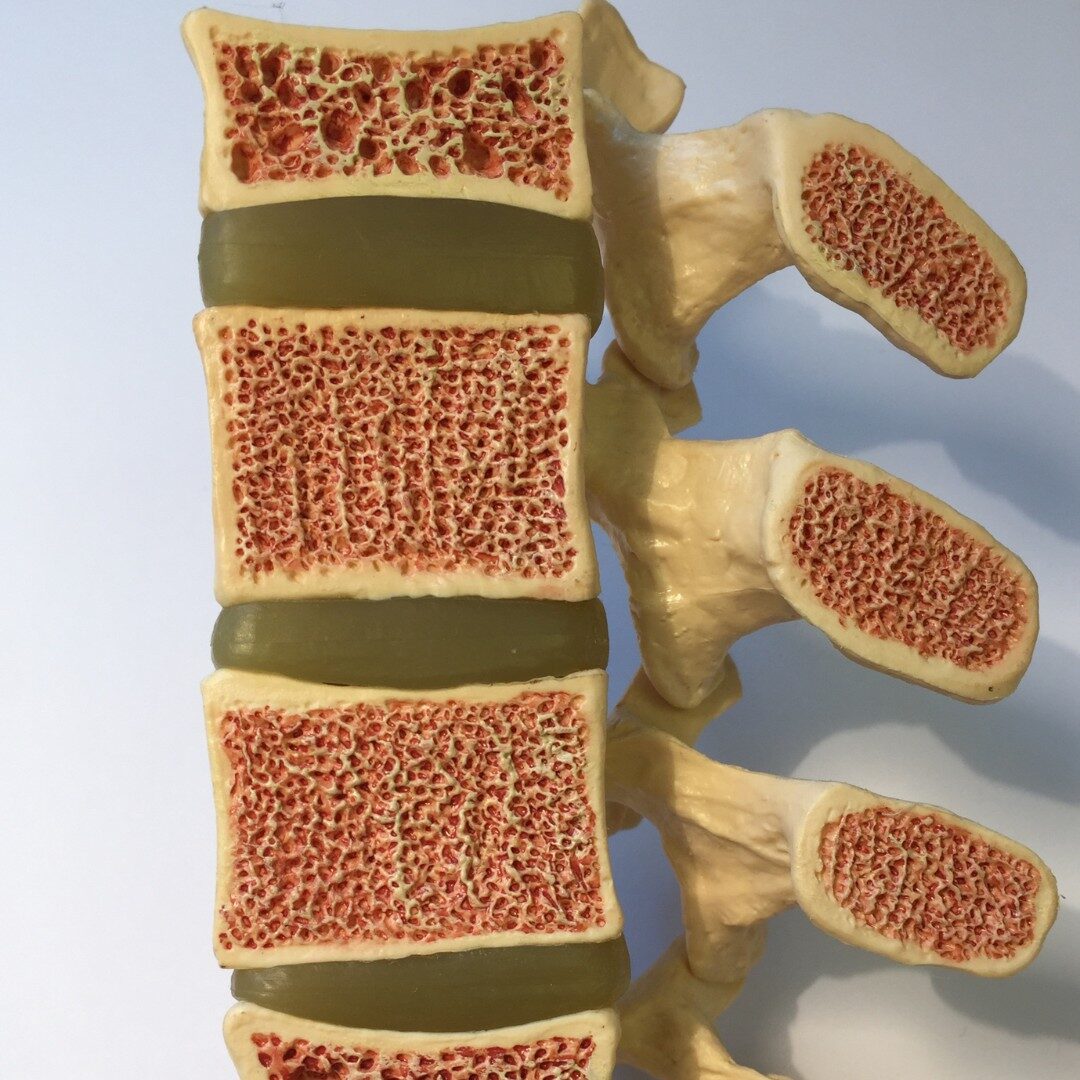
Osteoporosis
May 14, 2026
Osteoporosis and Menopause: How to Strengthen Your Bones and Prevent Bone Loss
Osteoporosis
October 17, 2025
World Osteoporosis Day is October 20: Here’s How to Strengthen Your Bones at Every Age
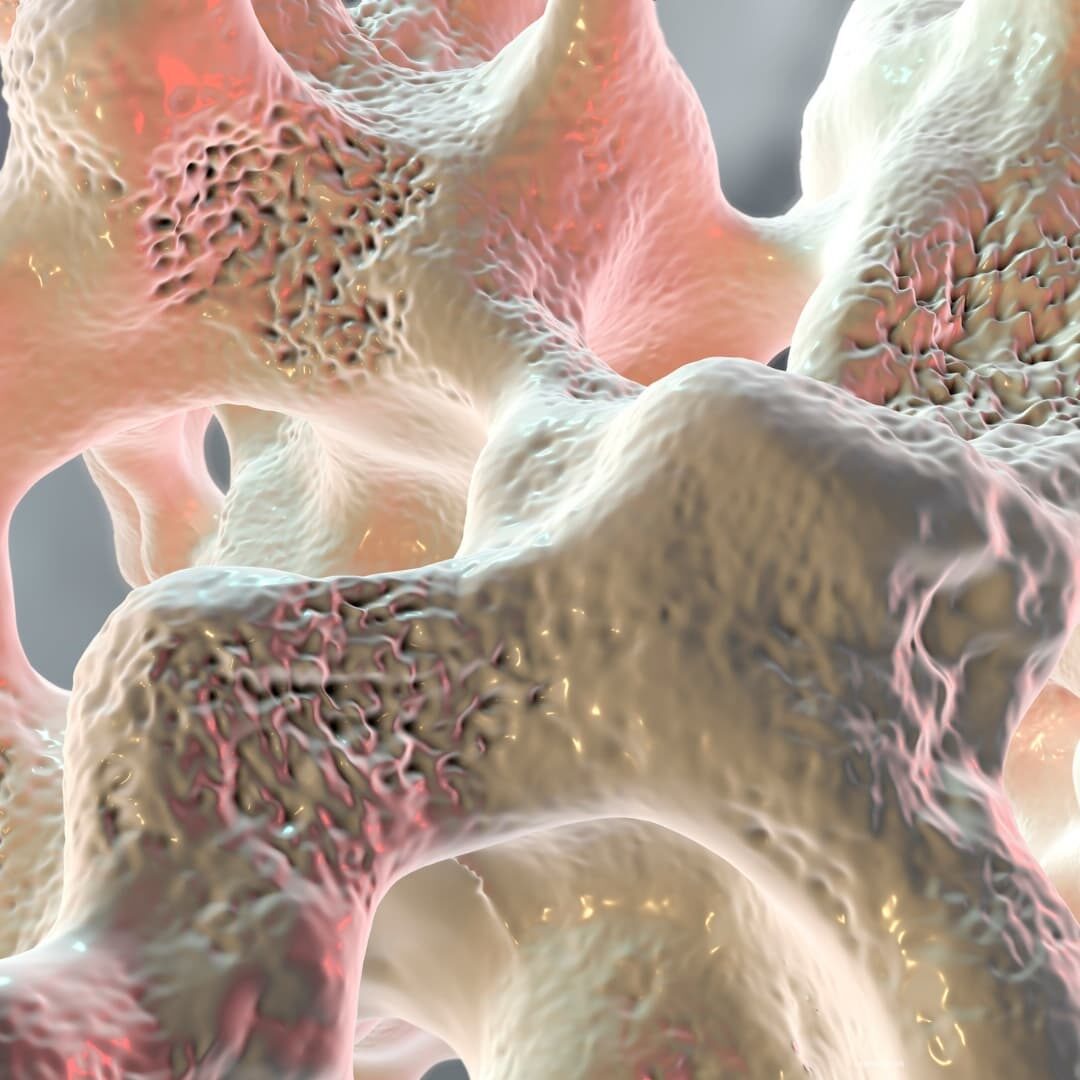
Osteoporosis
May 14, 2024
What’s the link between osteoporosis and the gut biome?
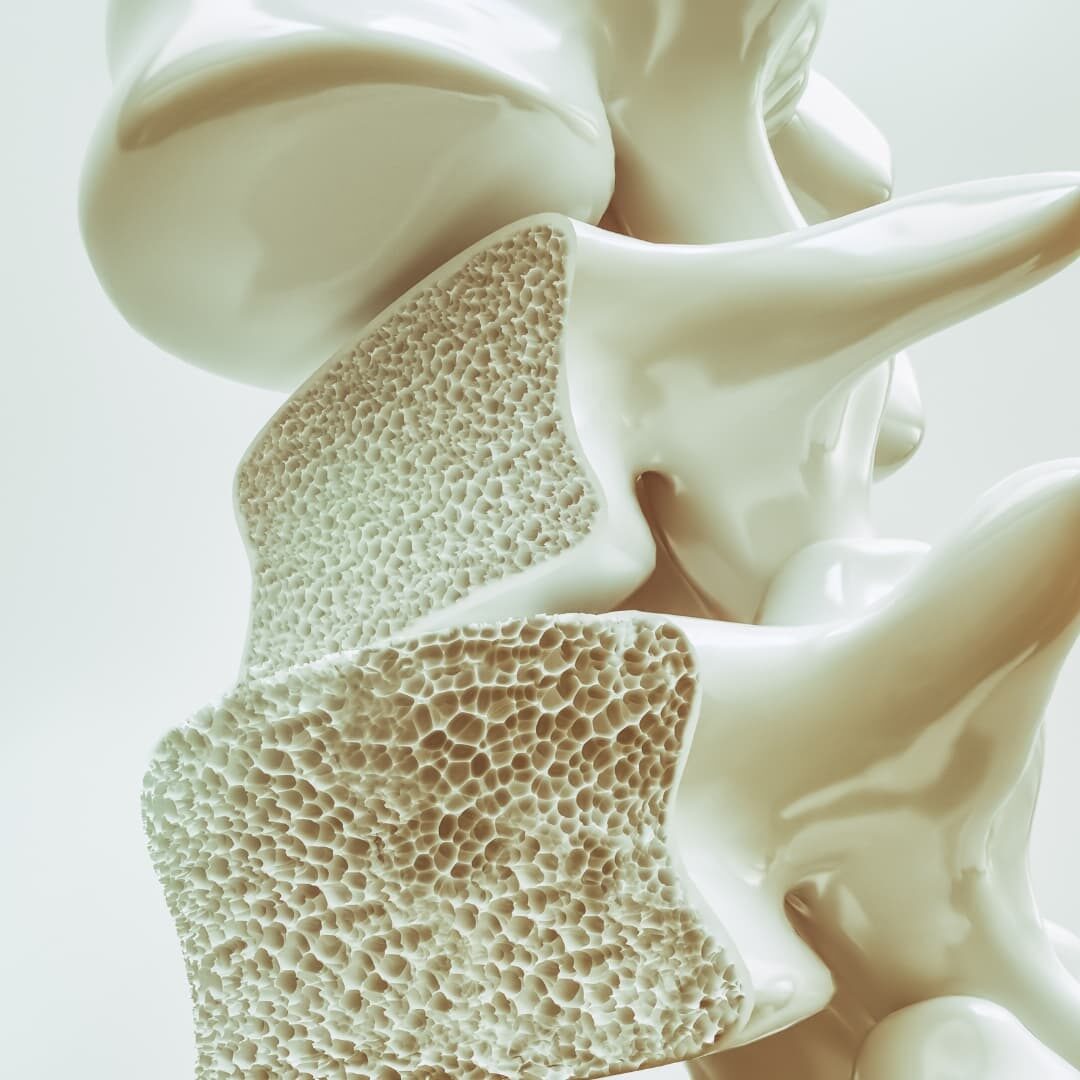
Osteoporosis
May 3, 2023
FAQs with Dr. Pandit: Osteoporosis